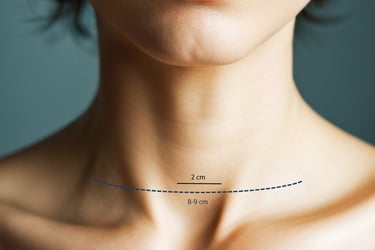
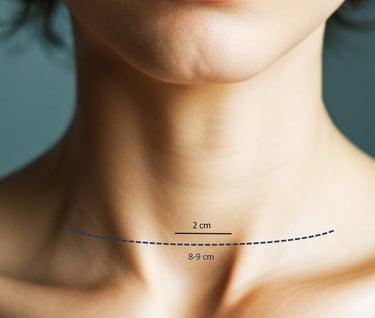
Minimally invasive video-assisted thyroidectomy - MIVAT
Minimally invasive thyroid surgery is designed for both benign pathology (thyroid nodules, graves disease) and for suspicious nodules or thyroid cancer confirmed by biopsy.
This technique allows surgery to resect half of the thyroid ("partial thyroidectomy") or total thyroidectomy.
In the case of a thyroid nodule, this must not exceed a maximum diameter of 4 mm, as larger nodules cannot be removed through the small incision through which the surgery is performed, and surgeons have to widen the incision to be able to remove the surgical specimen, thus losing the benefits of this technique
Minimally invasive video-assisted submaxilectomy - MIVAS
Submaxillary glands, located below the angle of the jaw, are salivary glands, responsible for most of the saliva we generate. Submaxillary pathology includes nodules, tumours (Warthin's tumour being the most frequent), lithiasis or chronic inflammation.
MIVAS is a technique developed and described for the first time by Dr. Parente, which allows the gland to be removed safely and through an aesthetically invisible approach.
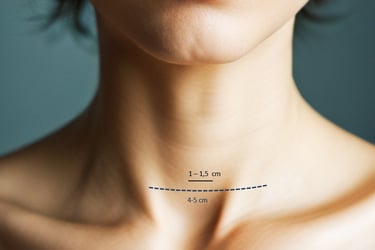
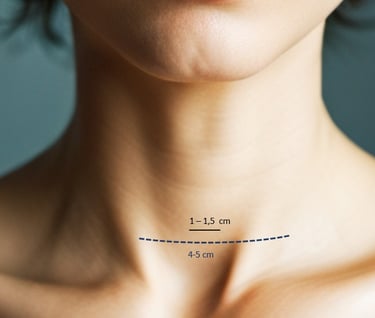
Minimally invasive video-assisted parathyroidectomy - MIVAP
Parathyroid glands are four small (0.5 cm) glands located behind the thyroid gland. Parathyroid surgery is performed in cases of overproduction of parathyroid hormone (PTH). This may be due to overgrowth of one of the glands (parathyroid adenoma) or hormone overproduction in all four glands (parathyroid hyperplasia).
With the MIVAP technique, either one parathyroid adenoma can be operated (previously localised by ultrasound and scintigraphy), or three of the four glands can be excised in cases of hyperplasia, through an incision of just 1 cm. Given that the half-life of PTH in the body is about 5 minutes, serial analyses are carried out during surgery to check that the hyperproduction of the hormone has stopped when the affected gland is removed, verifying the success of the technique.
About endoscopic neck surgery
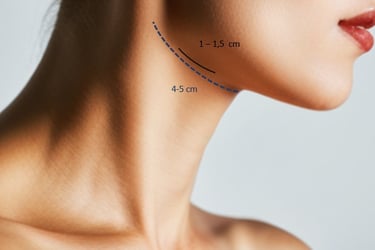
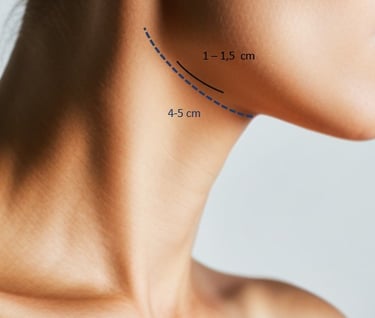
Endoscopic neck surgery is a novel surgical technique that has been developed over the last 20 years to improve the results of traditional neck surgery. With minimally invasive techniques and the use of the latest advances in endoscopic imaging, a significant improvement is achieved both in postoperative discomfort and in the incidence of surgical complications.
Due to the very small size of the incision, between 1 and 2 cm, the aesthetic result is optimal within a few weeks, being invisible a few months after surgery.
Find Us:
Servicio ORL - Hospital HM Rosaleda
C/ Rua de Santiago León de Caracas 1, 15701
Santiago de Compostela, España
Tlfn: +34 981551200 Ext 1016/1017

